Wrist Fusion
Mr Mike Hayton
FRCS (Trauma and Orth) FFSEM (UK)
Consultant Orthopaedic Hand Surgeon
A wrist fusion can be a very effective operation for controlling pain in an arthritic wrist. Arthritis can arise as a consequence of a number of conditions, including trauma, generalised wear and tear arthritis, inflammatory arthritis, such as those caused by rheumatoid arthritis or psoriasis.
Arthritis is a disease process whose end product is destruction of the articular cartilage of the joints. The articular cartilage is the slippery substance found at the end of bones. These allow the two bones in a joint to move with each other without any friction. In arthritis the cartilage is destroyed and the bone is exposed, and rubs against the opposite exposed bone surfaces, causing significant pain.
Why does it occur?
Arthritis can occur in a wrist as a consequence of a fracture that may have gone into the joint and healed with a step, causing localised wear and tear. Arthritis can occur as a generalised wear and tear process, with increasing age. Arthritis can occur as a consequence of inflammatory joint disease such as rheumatoid arthritis or psoriatic arthritis.
Symptoms
Patients often complain of pain and a decreased range of movement in the wrist. Painful actions include lifting and bending the wrist. These can be quite painful. Restricted range of movements can affect patients, with inability to perform common day-to-day tasks.
Clinical examination
Generally speaking the arthritic wrist is swollen and has a restricted range of movement.
Investigations
Plain x-rays often confirm the diagnosis, but further imaging such as a CT scan or MRI scan may visualise the joint space more carefully.
Non-operative treatment
Options could include splintage, to keep the wrist still, or x-ray guided cortico-steroid injections.
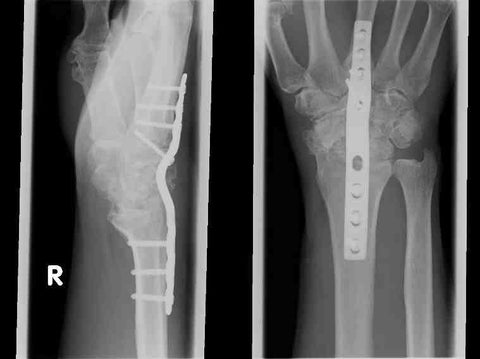
Operative treatment for wrist arthritis
There are two main types of fixation for wrist fusions. The first is a contoured plate that is held across the back of the wrist joint, with screws into the bone to secure fixation. The surgeon will carefully remove the remaining articular cartilage from the wrist joint to allow the bone to completely solidify underneath the plate. The second type of fixation is a pin that is passed across the wrist joint (usually down through the middle knuckle joint). This second type of fixation is often performed for patients with rheumatoid arthritis.
Post-operative rehabilitation
If a plate fixation is used and the fixation is solid often no post-operative immobilisation is required, and patients are advised to move their fingers as soon as possible. Swelling is common after such a surgery and it is advisable to highly elevate the hand for the first few weeks after surgery. If a pin fixation has been used then often this is supplemented with plaster of Paris for four to six weeks until the underlying bones have solidly united.
Return to activities of daily living
These, generally speaking, can be well tolerated with a plate fixation within the first two to three weeks. Heavy loading activities should be avoided until the bone has completely solidified.
Complications
The main risk is that of non-union, whereby the bone ends fail to completely grow over. This will cause the metalwork eventually to fail and the procedure may need to be repeated. With my technique this is very rare and occurs in less than 5% of fusions
General complications of wrist surgery can be viewed by clicking here